Musa Y. Tula 1*; Joel Filgona 2; Osaretin Iyoha 3; Usman U. Wafari 4; Richard Elisha 5
1, Department of Biological Science Technology, Federal Polytechnic Mubi, Mubi, Adamawa State, Nigeria
2, Department of Microbiology, Adamawa State University, Mubi, Adamawa State, Nigeria
3, Department of Medical Microbiology, School of Medicine, College of Medical Sciences, University of Benin, Benin City, Nigeria
4, Department of Food Science Technology, Federal Polytechnic Mubi, Mubi, Adamawa State, Nigeria
5, Department of Biomedical and Pharmaceutical Science Technology, Federal Polytechnic Mubi, Mubi, Adamawa State, Nigeria
E-mail:
birtyty@gmail.com
Received: 03/08/2022
Acceptance: 01/09/2022
Available Online: 02/09/2022
Published: 01/10/2022
Manuscript link
http://dx.doi.org/10.30493/DLS.2022.354292
Abstract
Detecting carbapenem-resistant Gram-negative bacteria with metallo-β-lactamase (MBL) producing traits in hospital fomites with no record of carbapenem use constitutes a serious challenge to the healthcare facility. This challenge results from the MBL capability of hydrolyzing all beta-lactams, including carbapenems, complicating antibiotic treatment. In this research, 100 samples comprising 77 hospital fomites (including sinks, beddings, door handles, and benches) and 23 swabs from the hands of healthcare workers from children, female and male wards of Mubi General Hospital were analyzed for Gram-negative bacterial growth. The Gram-negative isolates were screened for imipenem resistance and MBL production phenotypically by the combined disk test (CDT) method. The results showed that of all the Enterobacteriaceae isolates and Pseudomonas aeruginosa recovered from the hospital environment, only 5 (12.2%) were resistant to imipenem. These includes Escherichia coli (n=2), Pseudomonas aeruginosa (n=2) and Shigella species (n=1). From the isolates that were imipenem resistant, only three were phenotypically MBL producers, accounting for the prevalence of 7.3%, with an isolate each of P. aeruginosa, E. coli, and Shigella species. Though the occurrence of Gram-negative bacteria with MBL-producing traits in this hospital environment is low, the detection of such organisms in the hospital environment is worrisome because there is no account of carbapenem usage in the hospital, and the gene that encodes the production of the MBL enzymes are often carried on large mobile genetic elements.
Keywords: Carbapenem, Metallo-β-Lactamase, Gram-negative bacteria, Combined disk test
Introduction
The rate at which bacterial isolates, particularly members of the Enterobacteriaceae and Pseudomonadaceae families, are becoming increasingly resistant to commonly used antibiotics calls for concern. Beta-lactams are the commonly used antibiotics for therapy against the most severe diseases caused by the bacterial species of these families. The most potent of the beta-lactams is the carbapenem, which is often promoted for therapy against diseases caused by extended-spectrum-beta-lactamase (ESBL)-producing organisms, especially among species of Enterobacteriaceae and Pseudomonadaceae [1].
Resistance to beta-lactam antibiotics is thought to be mediated broadly by two mechanisms; those mediated by enzymes (such as extended-spectrum beta-lactamases and metallo-β-Lactamase), and non-enzymatic mechanisms (such as porin channel deletion and efflux pump) [1]. One of the most recognizable and documented mechanisms is the production of metallo-β-Lactamases (MBLs). Organisms that harbor transferrable MBL enzymes constitute a threat to therapy because the enzymes can break down beta-lactams, including carbapenems and inhibitors of beta-lactamases. The most concerning fact regarding MBL traits is that they are easily disseminated among bacteria of the same or different species since the gene that code for the MBL traits is most often borne on transferrable genetic elements [2]. In fact, infections involving MBL bacterial isolates are often difficult to detect and are correlated with high morbidity and mortality rates [3], aside from the limited therapeutic options and difficulty in treatment [4]. Thus, persistent infections involving MBL-producing organisms on the surfaces of hospital fomites and the hands of healthcare workers are not only a threat to therapy but may also affect quality healthcare delivery and impair the control and management of infections involving resistant bacterial isolates within healthcare settings [2].
Since infections involving MBL isolates are increasing worldwide, timely detection is crucial not only for appropriate and effective therapy but also for the execution of stringent measures to control their spread within hospital settings [5][6]. Although the use of molecular techniques to detect MBL bacterial isolates is the gold standard but is not available for routine use in most if not all of our hospitals. As such, using phenotypic methods, especially imipenem-EDTA combined disk, is cost-effective, simple, sensitive, and highly recommended [1]. Therefore, this study was undertaken to phenotypically unravel the presence of MBL-producing Gram-negative bacteria in non-clinical specimens from Mubi general hospital.
Materials and Methods
Study Area
This study was conducted at Mubi general hospital. The facility is situated in Mubi-South local government area of Adamawa State within the coordinates 10o15’54.9 N 13o16’10.0 E.
Sampling technique
Hundred non-clinical samples were collected from the hands of consented healthcare workers (23) and surfaces of hospital fomites (77), including sinks, beddings, door handles, and benches. The samples were collected using sterile swab sticks and were immediately introduced into appropriate differential bacteriologic media. The used media were MacConkey agar, Salmonella-Shigella agar, Eosin Methylene Blue agar, and Cetrimide agar. All media were incubated aerobically for 24hrs at 37 oC. Discrete colonies of the isolates were sub-cultured onto sterile nutrient agar slants and kept at refrigeration temperature for further use
Bacteria Identification
After Gram-staining, each bacterial isolate was identified on the Microgen A kit [7]. Each of these test kits is a plastic strip containing 12 microwells with dehydrated constituents that could identify 12 biochemical characteristics, namely lysine, ornithine, hydrogen sulfide production, glucose, mannitol, xylose, indole, urease production, Voges Proskauer, citrate utilization, tryptophan deaminase (TDA), and ortho-nitrophenol-β-galactoside (ONPG). The outcomes of the 12 (GN-A kit) microwell test strips after the addition of test isolate and 24 hrs incubation were converted to a 4 -digit octal code that was used to validate the identity of the tested bacterial isolate using Microgen ID computer software version 2.0.8.33. However, Pseudomonas aeruginosa was identified based on its reaction to the Cetrimide agar plate.
Screening for imipenem resistance
The Kirby-Bauer disk diffusion method was used to screen the identified bacterial isolates for imipenem resistance. For each bacterial suspension, 0.1ml corresponding to 0.5 McFarland standard was smeared on Mueller-Hinton agar (MHA) plates using a sterile swab stick, and an imipenem disk (10 µg) was positioned on the seeded plate and was kept at 35-37oC for 18-24 hrs in an incubator. Then, strains with an inhibition area diameter ≥23mm were considered sensitive, while strains with an inhibition zone diameter ≤19mm were taken as resistant [8]. The method was replicated on each bacterial isolate tested for confirmation.
Checking for Metallo-β-lactamase (MBL)
The presence or absence of MBL was screened among bacterial isolates resistant to imipenem by combined disk tests (CDT). In this method, two imipenem disks (10 µg each) were positioned 10-12 mm apart in a Mueller Hinton Agar (MHA) plate previously seeded with the test organism, and 10µl (750 µg) of 0.5 M EDTA solution, prepared by dissolving 18.6 g of the salt form to 100 ml and was adjusted to pH of 8.0 using NaOH, was added to one disc. The inhibition zone of ≥4 mm in diameter difference between imipenem disk + EDTA and imipenem disk alone was deduced as an affirmative result for MBL production [9]. The method was replicated on each bacterial isolate tested for confirmation.
Ethical consideration
Verbal informed consent was obtained from the healthcare workers of the hospital, and consent was sought and obtained from the management of the hospital. The hospital management and the participating healthcare workers were aware of the goal and objectives of the study.
Results
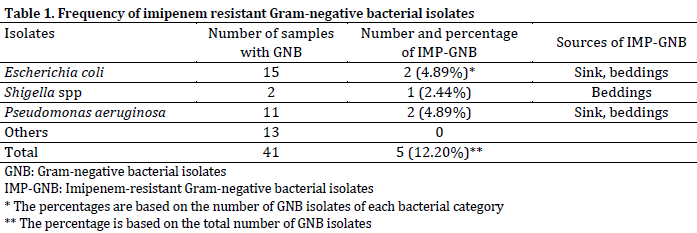
The results showed that of all the Enterobacteriaceae isolates and Pseudomonas aeruginosa recovered from the hospital fomites and the hands of healthcare workers, only 5 (12.2%) were resistant to imipenem and were taken as prospective Metallo-beta-lactamases (MBL) producers. These includes Escherichia coli (4.89%), Pseudomonas aeruginosa (4.89%) and Shigella species (2.44%) (Table 1).
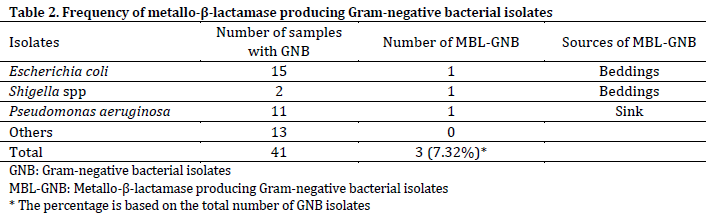
From the isolates that were imipenem resistant, only three were phenotypically MBL producers, accounting for the prevalence of 7.32%. These isolates were E. coli, P. aeruginosa, and Shigella, with one isolate each (Table 2).
Discussion
There are increasing reports of carbapenem-resistant Gram-negative bacteria (CR-GNB) in the hospital setting, its environment, and community-associated infections, which have wide-ranging implications for patient management. In this research, 5 out of the 41 bacterial isolates (12.2%) were imipenem-resistant Gram-negative bacteria. The low resistance to imipenem observed in this study was comparable to the 15.2%, 10.6%, and 10.2% carbapenem resistance reported in Lagos [10], Enugu [11], and Maiduguri [12], respectively. Additionally, the current observed resistant rates were comparable to other studies [13][14].
On the other hand, lower resistance to imipenem (7.37%) was also recorded [15]. However, higher resistance rates were reported in Malaysia [9] and Nepal [16], with 29.2% and 18.9% resistance rates, respectively. Nationally, higher rates of 28.2%, 28.6%, and 36.8% carbapenem resistance among Gram-negative bacteria were also reported in Sokoto [17], Enugu [18], and Lagos, Nigeria [19]. More so, excessive resistance rates of 82% [20] and 100% [21] were reported in Iran and China, respectively.
The isolation of imipenem-resistant Gram-negative bacteria from the hospital environment concurs with a report showing an extensive reservoir of the carbapenem-resistant organism in hospitals environment [17][22]. However, the low resistance to imipenem in this study could be due to its high cost and unavailability in healthcare settings and pharmacies of the studied area, which limit its misuse and excessive use. Therefore, bacterial isolates exhibited low or no resistance against it.
The phenomenon of cross-resistance could be the reason behind the isolation of CR-GNB in the study area with no previous record of carbapenem exposure. This phenomenon occurs when an organism gains resistance to an antibiotic to which it was not exposed. This phenomenon could be enhanced by the careless and widespread use of beta-lactam antibiotics in local healthcare facilities and communities. Furthermore, the observed resistant isolates in the current study could have been introduced by individuals in search of better healthcare delivery coming back from other countries where CR-GNB is endemic, as advocated by previous studies [17][23][24]. Additionally, most carbapenemase genes are carried on transferrable genomic elements, making it convenient for bacteria in a hospital environment to acquire and disseminate such coding genes successfully and easily [17][25].
The present study documented MBL-producing Gram-negative bacteria when the diameter of inhibition around imipenem + EDTA disk evaluated against imipenem disk alone was >4 mm. Previous studies reported that phenotypic methods, especially the CDT in which imipenem and EDTA are used, have high sensitivity and specificities to detect MBL-producing Gram-negative bacteria, similar to polymerase chain reactions (PCR) [9].
The occurrence of heritable MBLs among Gram-negative bacteria has eventually evolved globally and is gaining ground [26]. Similar to the finding of this research, several studies have reported the detection of MBL-producing organisms among imipenem-resistant Gram-negative bacteria by a combined disk test [9][27], particularly Pseudomonas spp., and E. coli [28]. However, the detection of the MBL trait among Shigella species in this study is novel and connotes the possible role of the transferrable genomic element in the study area.
MBL-producing organisms are often viewed as multidrug-resistant since they can inhibit the activities of a wide range of potent antimicrobials [29]. This resistance is enhanced by the presence of mobile genetic elements harboring the encoding genes. Studies have shown that the transferable genomic materials that carry the encoding genes for carbapenemase may also carry genes that bestow inhibitory activity against other classes of antimicrobials, resulting in the emergence of bacterial isolates with multidrug-resistant attributes. These organisms have limited therapeutic options, and the infections they cause may only be managed by expensive and slightly toxic antimicrobials. Therefore, numerous scientists have predicted the possible evolution of an era in which antimicrobials would no longer be effective against infections caused by microbial agents [29-31]. As such, the detection of Gram-negative bacteria with MBL-producing traits on the surfaces of hospital fomite in the current study with no records of carbapenem use is of public and clinical concern.
Conclusion
This study revealed the evolution and a low prevalence in the expression of metallo-β-lactamases among carbapenem-resistant Gram-negative bacteria from hospital fomites in a hospital with no records of carbapenem use. Therefore, urgent execution of programs that would ensure appropriate prescription and adequate use of antibiotics in the clinical and public settings, including measures that will impede the widespread dissemination of these types of organisms in the healthcare environment is imperative to contain this emerging threat.
References
| 1 | Yong D, Toleman MA, Giske CG, Cho HS, Sundman K, Lee K. Characterization of a new Metallo-βlactamase gene, blaNDM-1, and a novel erythromycin esterase gene carried on a unique genetic structure in Klebsiella pneumoniae Sequence Type 14 from India. Antimicrob. Agents Chemother.2009;53:5046–54. DOI |
| 2 | Behera B, Mathur P, Das A, Kapil A, Sharma V. An Evaluation of four different phenotypic techniques for detection of Metallo-β-lactamase producing Pseudomonas aeruginosa. Indian J. Med. Microbiol. 2008;26,233–7. DOI |
| 3 | Walsh TR, Toleman MA, Poirel L, Nordmann P. Metallo-beta-lactamases: the quiet before the storm? Clin. Microbiol. Rev. 2005;18:306-25. DOI |
| 4 | Peleg AY, Franklin C, Bell JM, Spelmann DW. Dissemination of the Metallo-β-lactamase gene blaIMP4 among gram-negative pathogens in a clinical setting in Austria. Clin. Infect. Dis. 2005;41:1549–56. DOI |
| 5 | Luzzaro F, Endimiani A, Docquier JD, Mugnaioli C, Bonsignori M, Amicosante G. Prevalence and characterization of metallo-beta-lactamases in clinical isolates of Pseudomonas aeruginosa. Diagn. Microbiol. Infect. Dis. 2004;48:131-5. DOI |
| 6 | Nordmann P, Poirel, L. (2002). Emerging carbapenemases in gram-negative aerobes. Clin. Microbiol. Infect.2002;8,321–31. DOI |
| 7 | Tula MY, Enabulele OI, Ophori EO, Aziegbemhin SA, Iyoha O, Filgona J. Phenotypic and molecular detection of multi-drug resistant Enterobacteriaceae species from water sources in Adamawa-North senatorial zone, Nigeria. Dysona Life Sci. 2022;3(2):57-68 DOI |
| 8 | Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. CLSI supplement M100. 2017. |
| 9 | Fahim Q, Khalid A, Hameed F, Sawed M. An inexpensive method of preparing EDTA disks for the detection of MBL in uropathonic E. coli. Pak. J. Pathol. 2018;29(4):72-5 |
| 10 | Oduyebo O, Falayi O, Oshun P, Ettu A. Phenotypic determination of carbapenemase-producing Enterobacteriaceae isolates from clinical specimens at a tertiary hospital in Lagos. Nig. Postgrad. Med. J.2015;22(4):223-7. DOI |
| 11 | Agbo E, Eze E. Phenotypic detection of Metallo-beta-lactamases production in imipenem resistant isolates of Escherichia coli and Klebsiella species isolated from hospital and environmental sources in Nsukka, Enugu State, Nigeria. J. Biol. Nat. 2015;2(4):135-41. |
| 12 | Mohammed Y, Zailani SB, Onipede AO. Characterization of KPC, NDM, and VIM type carbapenem resistance Enterobacteriaceae from North Eastern Nigeria. J. Biosci. Med. 2015;3:100-7. DOI |
| 13 | Jena J, Debata NK, Sahoo RK, Gaur M, Subudhi E. Genetic diversity study of various β-lactamase-producing multidrug-resistant Escherichia coli isolates from a tertiary care hospital using ERIC-PCR. Indian J. Med. Res. 2017;146:23. DOI |
| 14 | Wadekar MD, Anuradha K, Venkatesha D. Phenotypic detection of ESBL and MBL in clinical isolates of Enterobacteriaceae. Int. J. Curr, Res. Acad. Rev. 2013;1:89-95. |
| 15 | Yasdav KK, Adhikari N, Khadka R, Pant AD, Shah B. Multidrug-resistant Enterobacteriaceae and extended-spectrum β-lactamase producing Escherichia coli: a cross-sectional study in National Kidney Center, Nepal. Antimicrob. Res. Infect. Cont.. 2015;4:42. DOI |
| 16 | Bora A, Sanjana R, Jha BK, Mahaseth SN, Pokharel K. Incidence of Metallo-Beta-lactamase producing clinical isolates of Escherichia coli and Klebsiella pneumoniae in central Nepal. BMC Res. Notes, 2014;55:1-7. DOI |
| 17 | Olowo-okere A, Abdullahi MA, Ladidi BK, Suleiman S, Tanko N, Ungokore HY, Aliyu A. Emergence of Beta-Lactamase producing Gram-negative bacteria in a hospital with no history of Carbapenem usage in North-West Nigeria. Ife J. Sci. 2019;21(2):323-31. DOI |
| 18 | Chika E, Malachy U, Ifeanyichukwu I, Peter E, Thaddeus G, Charles E. Phenotypic detection of Metallo-β-lactamase (MBL) enzyme in Enugu, Southeast Nigeria. Amer. J. Biol. Chem. Pharma. Sci. 2014;2:1-6. |
| 19 | Enwuru NV, Enwuru CA, Adepoju-Bello A. Metallo-beta-Lactamase production by Escherichia coli and Klebsiella species isolated from hospital and community subjects in Lagos, Nigeria. Nat. Sci. 2011;9:1-9. |
| 20 | Rezai MS, Salehifar E, Rafiei A, Langaee T, Rafati M, Shafahi K, Eslami G. Characterization of multidrug-resistant extended-spectrum beta-lactamase-producing Escherichia coli among uropathogens of pediatrics in North of Iran. BioMed. Res. Int. 2015:1-7. DOI |
| 21 | Liang WJ, Liu HY, Duan GC, Zhao YX, Chen SY, Yang HY, Xi YL. Emergence and mechanism of carbapenem-resistant Escherichia coli in Henan, China 2014. J. Infect. Pub. Health, 2018;11(3):347-51. DOI |
| 22 | Gordon AE, Mathers AJ, Cheong EY, Gottlieb T, Kotay S, Walker AS, Stoesser N. The hospital water environment a reservoir for carbapenem-resistant organisms causing hospital-acquired Infections? A systematic review of the Literature. Clin. Infect. Dis. 2017;64(10),1435–44. DOI |
| 23 | Okeke IN, Edelman R. Dissemination of antibiotic-resistant bacteria across geographic borders. Clin. Infect. Dis. 2001;33:364–9. DOI |
| 24 | Leangapichart T, Rolain J, Memish ZA, Altawfiq JA, Gautret P. Emergence of drug-resistant bacteria at the Hajj: A systematic review. Travel Med. Infect. Dis. 2017;18:3–17. DOI |
| 25 | Potter RF, Alaric WD, Dantas G. The rapid spread of carbapenem-resistant Enterobacteriaceae. Drug Res. Updat. 2016;29:30-46. DOI |
| 26 | Bebrone C. Metallo-beta-lactamases (classification, activity, genetic organization, structure, zinc coordination) and their superfamily. Biochem. Pharmacol. 2007;74:1686-701. DOI |
| 27 | Farzana R, Shamsuzzaman SM, Mamun KZ. Isolation and molecular characterization of New Delhi Metallo-beta-lactamase-1 producing superbug in Bangladesh. J. Infect. Dev. Countries, 2013;7(3):161-8. DOI |
| 28 | Hsu LY, Apisarnthanarak A, Khan E, Suwantarat N, Ghafur A, Tambyah AP. Carbapenem-Resistant Acinetobacter baumannii and Enterobacteriaceae in South and Southeast Asia. Clin. Microbiol. Rev. 2017;30(1):1-22. DOI |
| 29 | Meini MR, Llarrull LI, Vila AJ. Evolution of Metallo-β-lactamases: Trends Revealed by Natural Diversity and in vitro Evolution. Antibiotics, 2014;3:285-316. DOI |
| 30 | Smith R, Coast J. The true cost of antimicrobial resistance. Brit. Med. J. 2013;346:1493. DOI |
| 31 | McKenna M. Antibiotic resistance: The last resort. Nat. 2013;499:394–6. DOI |
Cite this article:
Tula, M., Filgona, J., Iyoha, O., Wafari, U., Elisha, R. Screening of hospital fomites and hands of healthcare workers for Metallo-β-Lactamase producing Gram-negative bacteria in Mubi general hospital Nigeria. DYSONA – Life Science, 2022;3(2): 76-81. doi: 10.30493/dls.2022.354292